Anatomy of the Upper Limb ( Part - 1 ) : Fmge, Neet pg, NEXT and USMLE Step 1
Dr.G Bhanu Prakash Animated Medical Videos・82 minutes read
Anatomy lecture on clavicle, scapula, and humerus focusing on landmarks, fractures, and nerve injuries to prepare students for exams and clinical practice. Topics include muscles related to the chest, breast anatomy, and internal thoracic artery supply, aiding in comprehension for first to third-year students.
Insights
- The clavicle is a unique bone in the body due to its S-shape, subcutaneous location, and early ossification during the fifth and sixth week of intrauterine life, making it the first bone to ossify. The most common site of clavicular fractures is at the junction between the medial three-fifths and lateral two-fifths, highlighting its clinical significance.
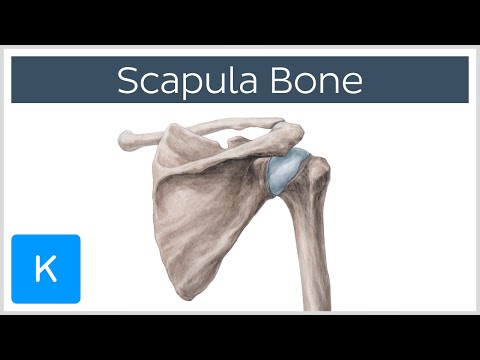
- The scapula features distinct structures like the spine, acromion process, coracoid process, and glenoid cavity, extending from the second to the seventh posterior rib. Understanding developmental aspects, such as the descent of the scapula during the 9th to 12th week, is crucial, as conditions like Klippel-Feil syndrome can result in congenitally high scapula known as Pringle deformity.
- Muscles like pectoralis major and minor, serratus anterior, and external oblique play significant roles in the upper limb, with nerves like the long thoracic nerve innervating serratus anterior. Clinical conditions like Poland syndrome and the importance of structures like the clavipectoral fascia in exams underscore the practical applications of anatomical knowledge.
Get key ideas from YouTube videos. It’s free
Recent questions
What is the structure of the clavicle bone?
The clavicle is an S-shaped bone, the only horizontal bone in the body, subcutaneous, and the first bone to ossify during the fifth and sixth week of intrauterine life. It has no medullary cavity, two ossification centers, and the most common site of fracture is the junction between medial three-fifths and lateral two-fifths.
What are the components of the scapula bone?
The scapula bone consists of a spine, acromion process, coracoid process, and glenoid cavity. It extends from the second to the seventh posterior rib, with the thickest border being the lateral border. To locate the coracoid process, palpate beneath the clavicle in the infraclavicular fossa.
What are the important landmarks of the humerus bone?
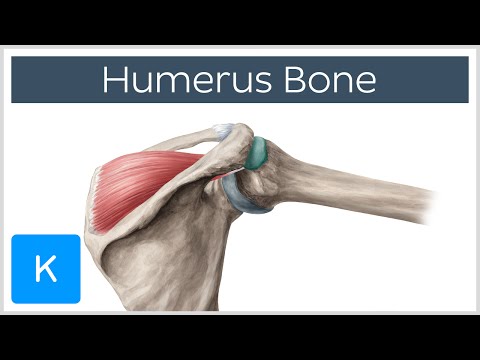
The humerus bone comprises the head, neck, and shaft, with greater and lesser tuberosities. It has anatomical and surgical necks, with the intertubercular sulcus located between the tuberosities. Nerve injuries associated with humeral fractures include the axillary nerve, anterior circumflex humeral artery, and posterior circumflex humeral artery.
What clinical conditions are associated with scapula abnormalities?
People with Klippel-Feil syndrome may have a high scapula due to improper descent, known as Pringle deformity. Understanding these conditions is crucial for identifying congenital abnormalities and their implications on musculoskeletal function.
What are the key muscles discussed in relation to the pectoral region?
Pectoralis major and minor, along with subclavius, are significant muscles in the pectoral region. Pectoralis major is attached to the clavicle and sternum, responsible for arm flexion, medial rotation, and adduction. Pectoralis minor divides the axillary artery and is crucial for vascular supply. Understanding these muscles aids in comprehending upper limb movements and clinical conditions related to nerve innervation.
Related videos

PW MedEd
Upper Limb - Anatomy | MBBS 1st Year | FARRE Series | Dr. Pradeep | PW MedEd

Kenhub - Learn Human Anatomy
Clavicle Bone - Location, Definition & Function - Human Anatomy | Kenhub

Blackriver & Bootsma Education
Identification of Bony Landmarks - Upper Extremity - Clavicle Scapula Humerus Ulna Radius Hand
Kenhub - Learn Human Anatomy
Anatomy and Function of the Scapula - Human Anatomy | Kenhub
Kenhub - Learn Human Anatomy
Humerus Bone - Anatomy, Definition & Function - Human Anatomy | Kenhub



Summary
00:00
Clavicle and Scapula Anatomy Lecture Summary
- Anatomy lecture focusing on clavicle and scapula
- Clavicle is an S-shaped bone, the only horizontal bone in the body
- Clavicle is subcutaneous and the first bone to ossify in the body
- Clavicle ossifies during the fifth and sixth week of intrauterine life
- Most common site of clavicular fracture is the junction between medial three-fifths and lateral two-fifths
- Clavicle has no medullary cavity and two ossification centers
- Sterno clavicular joint is a saddle joint, acromio clavicular joint is a plain synovial joint
- Clinical condition of hypoplastic clavicles can lead to cleidocranial dysostosis
- Scapula has a spine, acromion process, coracoid process, and glenoid cavity
- Thickest border of the scapula is the lateral border
18:42
Scapula and Humerus Anatomy Overview
- The scapula extends from the second posterior rib to the seventh posterior rib.
- To locate the coracoid process, palpate beneath the clavicle in the infraclavicular fossa.
- The coracoid process is an example of an atavistic epiphysis.
- During the 9th to 12th week of development, the scapula descends from the cervical region to the shoulder region.
- People with Klippel-Feil syndrome may have a congenitally high scapula due to the scapula not descending properly.
- The congenitally high scapula condition is known as Pringle deformity and is associated with Klippel-Feil syndrome.
- The humerus consists of the head, neck, and shaft, with the greater and lesser tuberosities.
- The anatomical neck and surgical neck of the humerus are important landmarks.
- The intertubercular sulcus, or bicipital groove, is located between the greater and lesser tuberosities.
- Nerve injuries associated with humeral fractures include the axillary nerve, anterior circumflex humeral artery, and posterior circumflex humeral artery.
36:27
Nerve Injuries in Fractures: Clinical Points
- The median nerve passes through the supracondylar region.
- Clinical points include identifying nerve passage areas and nerve injuries in fractures.
- In mid-shaft humerus fractures, the radial nerve is injured.
- Fractures of the medial epicondyle cause ulnar nerve injuries.
- Fractures in the supracondylar region lead to median nerve injuries.
- Workman's contracture occurs due to brachial artery compression, leading to muscle necrosis.
- Myositis ossificans results from calcium deposition in muscles due to tight wrapping.
- Practical quiz questions include identifying nerve injuries in specific fractures.
- Police fracture involves radial head displacement upwards, while Smith fracture involves downward displacement.
- Barton fractures can be dorsal or ventral, with displacement of the radial styloid process and radiocarpal joint.
56:01
Significance of Anatomy in Orthopedics Explained
- Anatomy is not typically taught in detail, but its importance is evident in Orthopedics and other subjects.
- Understanding the significance of anatomy is crucial in the first to third years of study.
- The discussion covers various topics to ensure clarity in understanding.
- A detailed explanation of fractures involving the radius and ulna is provided.
- Fractures such as Monteggia and Galeazzi fractures are explained with mnemonic aids.
- Practical tips on remembering fractures are shared, emphasizing location and characteristics.
- The importance of the annular ligament in preventing subluxation is highlighted.
- Detailed information on carpal bones, metacarpals, and phalanges is provided.
- Mnemonics are shared to aid in remembering the names and order of carpal bones.
- Common questions related to fractures, ossification, and dislocations are addressed, aiding in retention and understanding.
01:15:53
"Pectoral Muscles and Nerve Supply Overview"
- Serratus anterior is the next muscle to be taught, emphasizing the importance of understanding origins and insertions for third-year students.
- In upcoming exams, the focus will be on the actions of muscles, such as what happens if a muscle undergoes paralysis or if the nerve supplying it is affected.
- Pectoralis major and minor, along with subclavius, are discussed, with pectoralis major being the main chest muscle attached to the clavicle and sternum.
- Pectoralis minor is known as the "key muscle of the pectoral region" due to its role in dividing the axillary artery into three parts.
- The actions of pectoralis major include flexion, medial rotation, and adduction of the arm, making it a significant muscle in the upper limb.
- The long thoracic nerve innervates serratus anterior, also known as the boxer's muscle, and its paralysis can lead to winging of the scapula.
- Partial winging of the scapula is caused by damage to the spinal accessory nerve, affecting the trapezius muscle and leading to protraction of the scapula.
- The nerves supplying various muscles in the pectoral region are discussed, with routine questions focusing on lateral and medial pectoral nerves, nerve to subclavius, and long thoracic nerve to serratus anterior.
- Poland syndrome, characterized by chest wall hypoplasia due to the absence of pectoralis muscles unilaterally, is highlighted as a clinical condition.
- Clavipectoral fascia, located between the clavicle and pectoralis major muscle, is explained as a crucial topic likely to be tested in exams.
01:34:44
Anatomy of Clavipectoral Fissure and Breast
- The clavipectoral fissure is a structure between the clavicle and pectoralis minor, covered by clavipectoral fascia.
- In exams, students are asked about the structures piercing the clavipectoral fascia, including an artery, vein, nerve, and lymphatics.
- The structures piercing the clavipectoral fascia are the thoracoacromial artery, cephalic vein, lateral pectoral nerve, and lymphatics.
- Understanding these structures can secure one mark in exams.
- The mammary gland is a modified sweat gland with apocrine activity, located from the second to sixth rib.
- Dividing the breast into four quadrants, the superior lateral quadrant with the axillary tail of Spence has the highest risk of breast tumors.
- Muscles related to the breast include pectoralis major, serratus anterior, and external oblique muscles.
- The breast is located in the superficial fascia, with a retro mammary space containing loose areolar connective tissue.
- The nipple lies in the fourth intercostal space, surrounded by the areola with sebaceous glands called tubercles of Montgomery.
- The breast has 15 to 20 lobes, each opening into a lactiferous sinus and duct, with blood supply from the subclavian artery branching into the axillary artery.
01:55:42
Internal thoracic artery supplies breast and more
- The internal thoracic artery, also known as the internal mammary artery, supplies the mammary gland. It gives rise to branches such as the Superior thoracic artery, lateral thoracic artery, and acromiothoracic artery, along with posterior intercostal arteries that supply the breast.
- A mnemonic "SLAP" can help remember the branches supplying the breast: Superior thoracic, lateral thoracic, acromiothoracic, and posterior intercostal arteries. The left internal thoracic artery is commonly used for coronary artery bypass grafting.
- Further sessions will cover lymphatics, venous drainage, and muscles of the upper limb. Feedback is requested to ensure understanding and guide future classes, with a focus on first and third-year students. Tomorrow's session will concentrate on the upper limb, including topics like cubital fossa and carpal tunnel syndrome.




